


Volume Loss or Volume Shift?
"I think I've lost volume."
Patients often point to their cheeks or lips. They describe looking older, flatter or less supported than they once did. Some feel that their face appears tired, and others feel they have become hollow.
Sometimes they’re right, but one of the most important concepts in facial ageing is that apparent volume loss is not always true volume loss.
What Patients Mean By Volume Loss
When patients talk about volume loss, they are usually describing a visible change. Flatter cheeks, thinner lips. Their face might not reflect light the way it once did.
The concern is real, but the challenge is determining why it has occurred, because the face doesn’t age in a single layer. Changes affecting bone, fat compartments, ligaments and skin can all alter how volume appears.
Genuine Volume Loss Does Occur
Volume loss is a recognised part of facial ageing. Over time, some fat compartments lose volume and support. The facial skeleton also undergoes gradual remodelling. Together, these changes can reduce projection and alter facial contour. This is often most noticeable within the mid-face. Patients may observe flatter cheeks, increasing shadows beneath the eyes and reduced facial support. In these situations, volume loss is a genuine contributor to the ageing process.
Why Volume Can Appear To Disappear
Volume does not always disappear. Sometimes it moves (!). Certain fat compartments lose volume as we age, while others descend. This means a patient may simultaneously feel hollow in one area while appearing heavier in another. A flatter cheek may coexist with a more prominent nasolabial fold or jowls. This is one reason why facial ageing can feel confusing. The mirror suggests volume loss, but the anatomy often reveals a combination of volume loss and volume shift.
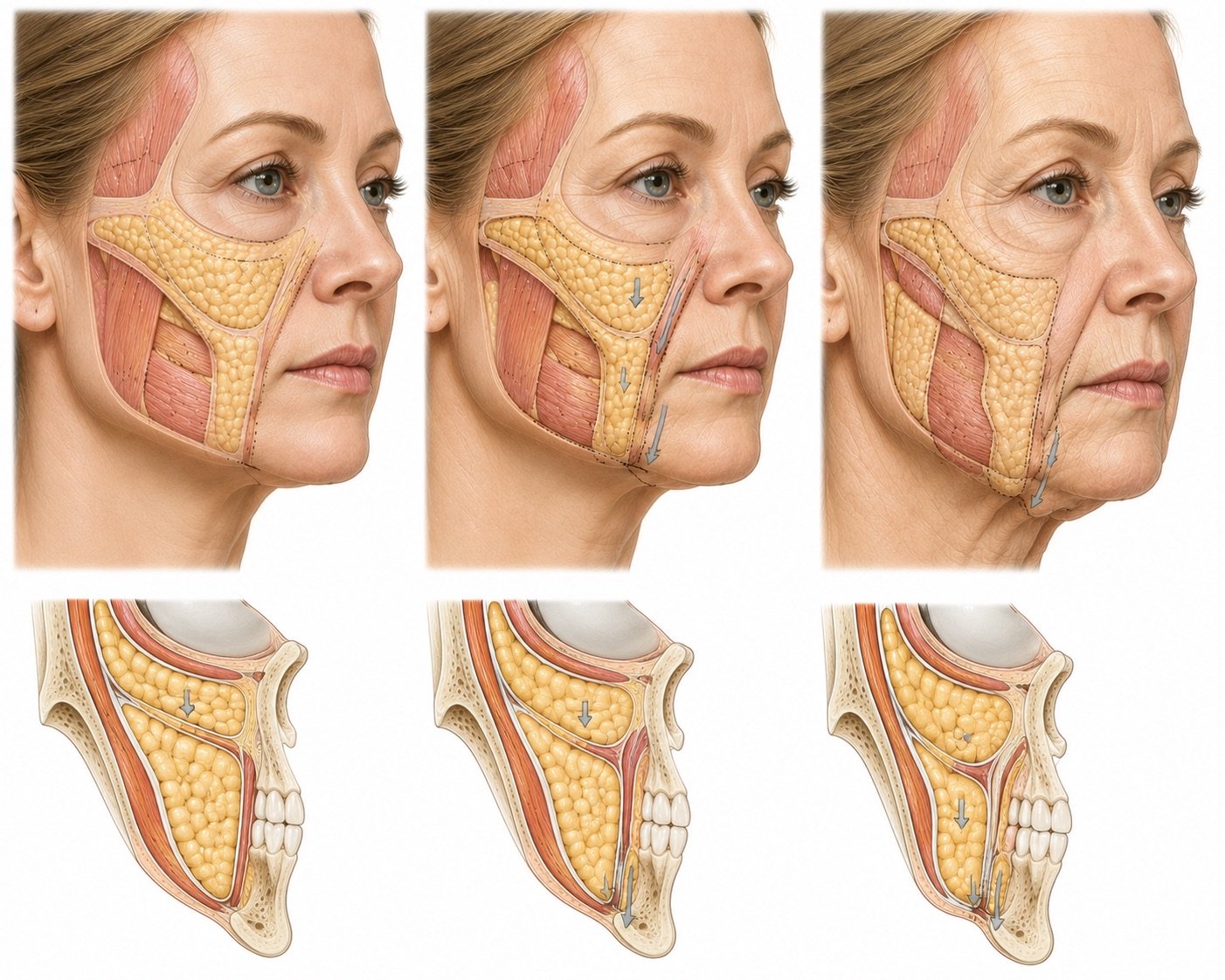
Why The Mid-Face Matters
When a patient tells me they have lost cheek volume, my assessment rarely begins with the cheek alone. I am looking at mid-face support.
I assess the effects of bone remodelling, fat compartment changes and the relationship between the cheek, under-eye region and lower face. Support often begins higher in the face. Changes within the mid-face can influence the appearance of the lower face. This is why assessment frequently starts with the structures responsible for support rather than the fold or hollow that first caught the patient's attention.
The Link Between The Mid-Face And The Lower Face
One of the biggest "aha" moments during consultation occurs when patients learn that restoring support within the midface may influence the appearance of other areas.
Patients often focus on the nasolabial folds or jowls because they’re the changes they notice the most. However, support lost higher in the face may contribute to what they are seeing lower down. In selected patients, improving structural support within the mid-face can soften the appearance of the mid and lower face without directly treating every visible feature.
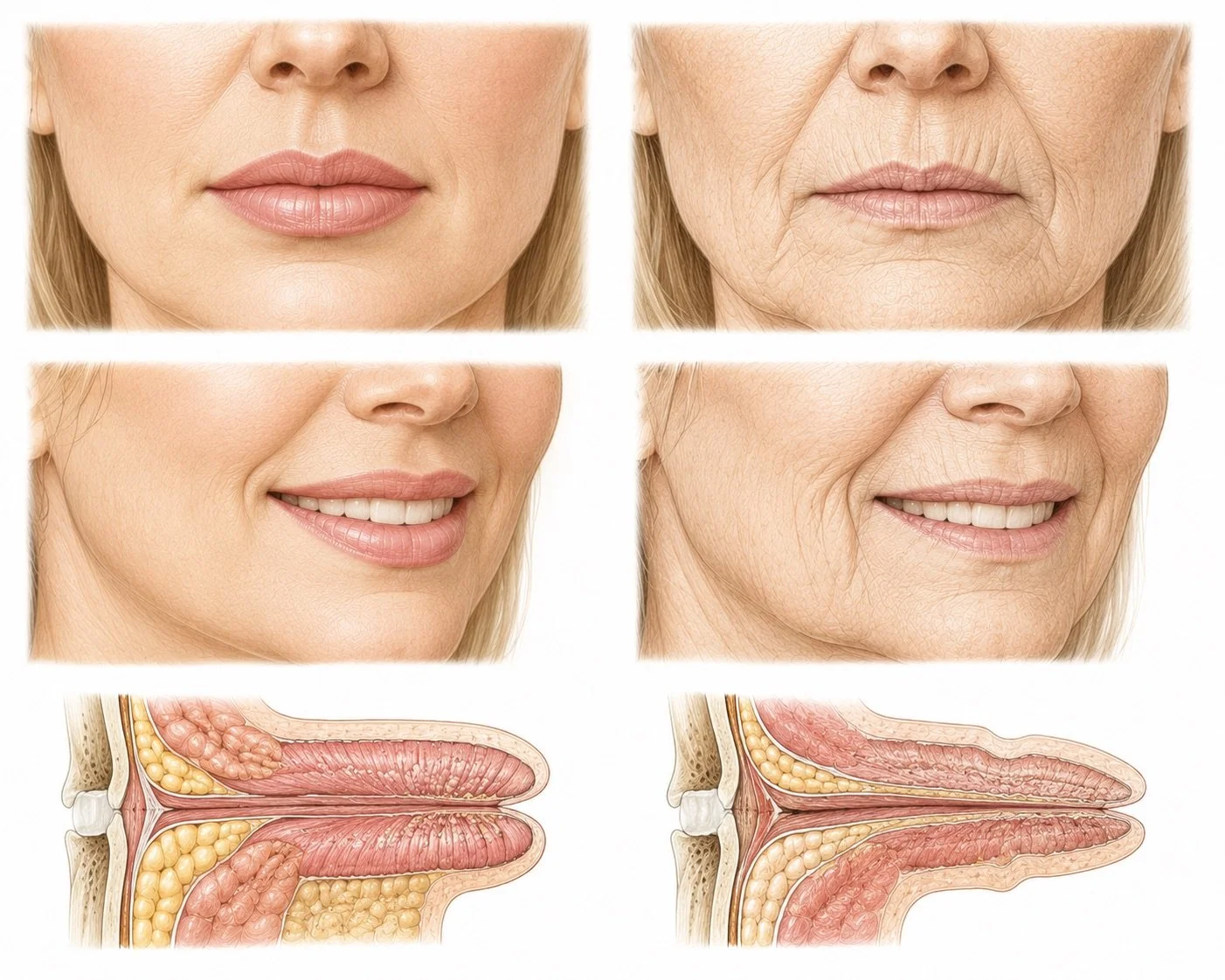
Lips Are A Different Conversation
Lip ageing deserves separate consideration. Many older patients experience genuine age-related volume loss within the lips. The lips may appear thinner, particularly during smiling. Lip definition may become less distinct. Perioral lines may become more apparent.
However, not every patient presenting with concerns about lip volume has actually lost volume. In patients who have undergone previous filler treatments, I occasionally find that volume remains present. Sometimes there may even be evidence of overfilling or filler migration. In these situations, the question is not always how to add more volume, but whether the existing volume remains appropriate. Maybe we should dissolve old work and reassess?
Why More Volume Is Not Always Better
One of the most common misconceptions in aesthetic medicine is that every sign of ageing reflects missing volume. This is rarely true. As I’ve already stated, structural ageing is influenced by changes in bone, fat compartments, ligaments and skin quality simultaneously.
Adding volume without understanding these changes may not move a patient closer to their goals. In some cases, additional volume may even create an appearance that feels less natural. This is why I generally approach treatment planning by asking a simple question: What is causing the appearance the patient is concerned about? Only after understanding the cause can a sensible treatment plan be developed.
A Doctor's Perspective
Patients are very good at recognising change. What is more difficult is identifying why that change has occurred. When a patient tells me they have lost volume, my first task is not deciding how to replace it, but to determine whether the issue is genuine volume loss, volume shift, declining structural support, changes in skin quality or a combination of all four, because facial ageing is rarely caused by a single process.
If patients take away one message from this discussion, I would like it to be this: Not every hollow reflects volume loss. Not every fold requires filling. And not every ageing concern is solved by adding more volume.